

Hypermobility in Kids: Normal or not?
By Nicole Pates | Paediatric Physiotherapist | Western Kids Health
If you have ever been told your child is “hypermobile” or “really bendy” and walked away thinking “OK… but what does that actually mean?” then you are not alone.
Maybe it came up at an OT appointment. Maybe a teacher mentioned it. Maybe you have noticed your child sits in unusual positions or seems way more flexible than their friends. And now you are Googling at midnight, finding a lot of acronyms and not a lot of clarity.
So let me break it down for you in plain language. Because most of the time, being bendy is completely normal. And when it is not, there are things we can do to help.
What is hypermobility?
Hypermobility simply means joints that move beyond the typical range. Think of it as being extra flexible. It is a feature of how your child’s connective tissue is built, and it is passed through families just like eye colour or hair colour.
It can show up in different ways. Some kids are flexible through lots of joints (generalised). Some are only flexible in specific areas like shoulders or knees (localised). And some just have really bendy fingers and hands (peripheral).
Hypermobility rates also vary across different ethnic backgrounds. We see higher prevalence in African, Asian, and Middle Eastern populations compared to Caucasian populations. So a child’s ethnic background is relevant when thinking about whether their level of flexibility is typical for them.
Around 10 to 25% of children worldwide show some degree of joint hypermobility. That range itself reflects the ethnic and geographic variation.

Is it normal?
Yes, most of the time. Babies, toddlers, and young children are naturally more flexible. Their bones are still developing and ossifying (wrist bones, for example, are not fully formed until around age 14), which means more movement at the joints. That flexibility is supposed to be there.
The Beighton Score: what is it (and what it isn’t)
The most commonly used screening tool for generalised joint hypermobility is called the Beighton score. It looks at flexibility across five areas: little fingers, thumbs, elbows, knees, and whether a child can place their palms flat on the floor with straight knees. Each item is scored as a simple yes or no, and the total is out of 9.

Really important: The Beighton score is not a severity scale. A child who scores 8 is not “more hypermobile” or “worse off” than a child who scores 6. Both meet the threshold for generalised joint hypermobility. The number tells us how many joints met the yes/no criteria, not how much impact the hypermobility is having on your child’s life. Two children can score the same number and have completely different experiences. One might be thriving in gymnastics. The other might be struggling with pain and fatigue.
It is also just a screen, not a diagnosis. A score below 6 does not rule out localised hypermobility in specific joints. Your child might score 4 on the Beighton but still have significantly hypermobile ankles or shoulders that are causing issues. And the score changes over time as children grow.
This screen is generally only meaningful from around age 5, because younger children are naturally very flexible and the Beighton is not reliable in that age group.
So will my child always be hypermobile?
For children, a score of 6 out of 9 or more suggests generalised joint hypermobility (GJH) – “extra bendy”. This cut-off was confirmed by a 2024 meta-analysis in the European Journal of Pediatrics, pooling data from over 28,000 children across 37 studies worldwide and represents kids 2 standard deviations above average – that pointy end of the bell curve (top 10%). In the past, cut-offs of 4 or 5 out of 9 were used to classify children as “generalise joint hypermobility” but now we have good quality research to show these numbers are too low, include lots of children and are no longer recommended. Please, when you read research, check what Beighton score cut off was used… because if it is too low, it will include children who do not have GJH.
And here is the really important bit: flexibility changes over time. A 2025 longitudinal study followed 126 children over two years and found that generalised hypermobility dropped from 25% to just 6%. A child who scores high on flexibility tests at age 7 might score much lower by age 9. Girls tend to stay flexible a bit longer than boys, and that is completely normal too.

Beighton score graph fromshowing mean total Beighton score decreasing over three measurement points for boys and girls
The bottom line: if your child is bendy but happy, active, and doing well, there is nothing to “fix.” They might sit in different positions. They might move in ways that look a bit different. That is just their body doing what works for them.
Can we diagnose kids with a hypermobility condition?
This is one of the most common questions I get. And the answer has shifted quite a bit in recent years.
The short version: we try not to give a fixed, lifelong diagnosis during childhood. But that does not mean we sit back and wait.
In 2023, the Paediatric Working Group of the International Consortium on EDS and Hypermobility Spectrum Disorders released a new diagnostic framework specifically for children (Tofts et al., 2023, Orphanet Journal of Rare Diseases). The big shift is that it recognises children’s bodies change significantly as they grow. Instead of locking in a label, the framework uses a sliding system where children can move between categories as they develop. You can view the full framework at ehlers-danlos.com.
It is important to understand that this criteria should only be used after ruling out other conditions. Hypermobility can be a feature of other heritable connective tissue disorders, including other subtypes of Ehlers-Danlos syndrome, Marfan syndrome, and Loeys-Dietz syndrome. Some of these have significant cardiac or vascular implications. A thorough family history and clinical assessment by a paediatrician or a rheumatologist is key to making sure we are not missing something that needs different management. The diagnostic framework specifically requires that other conditions are considered and excluded before classifying a child within the paediatric hypermobility categories.


Caption: Left: Hand x-ray, age 4. Right: Hand x-ray, age 14. Notice how many wrist bones are still forming at age 4. This is why screening is not meaningful before around age 5.
Here are a few key age markers to know about:
Under 5: Too young for formal diagnosis. Their bones are still ossifying, which means Beighton scores can change rapidly. But this does not mean we wait and see. If your child is struggling with movement, play, communication, or learning, we actively support them right now. Physiotherapy, occupational therapy, and speech pathology all have a role in helping your child move, play, talk, and learn. We document the hypermobility, we consider it in our clinical reasoning, and we give your child the best possible support if things are tricky. We just do not attach a fixed diagnostic label at this stage because the picture is still developing. If things are really tricky we work with your paediatrician or rheumatologist.
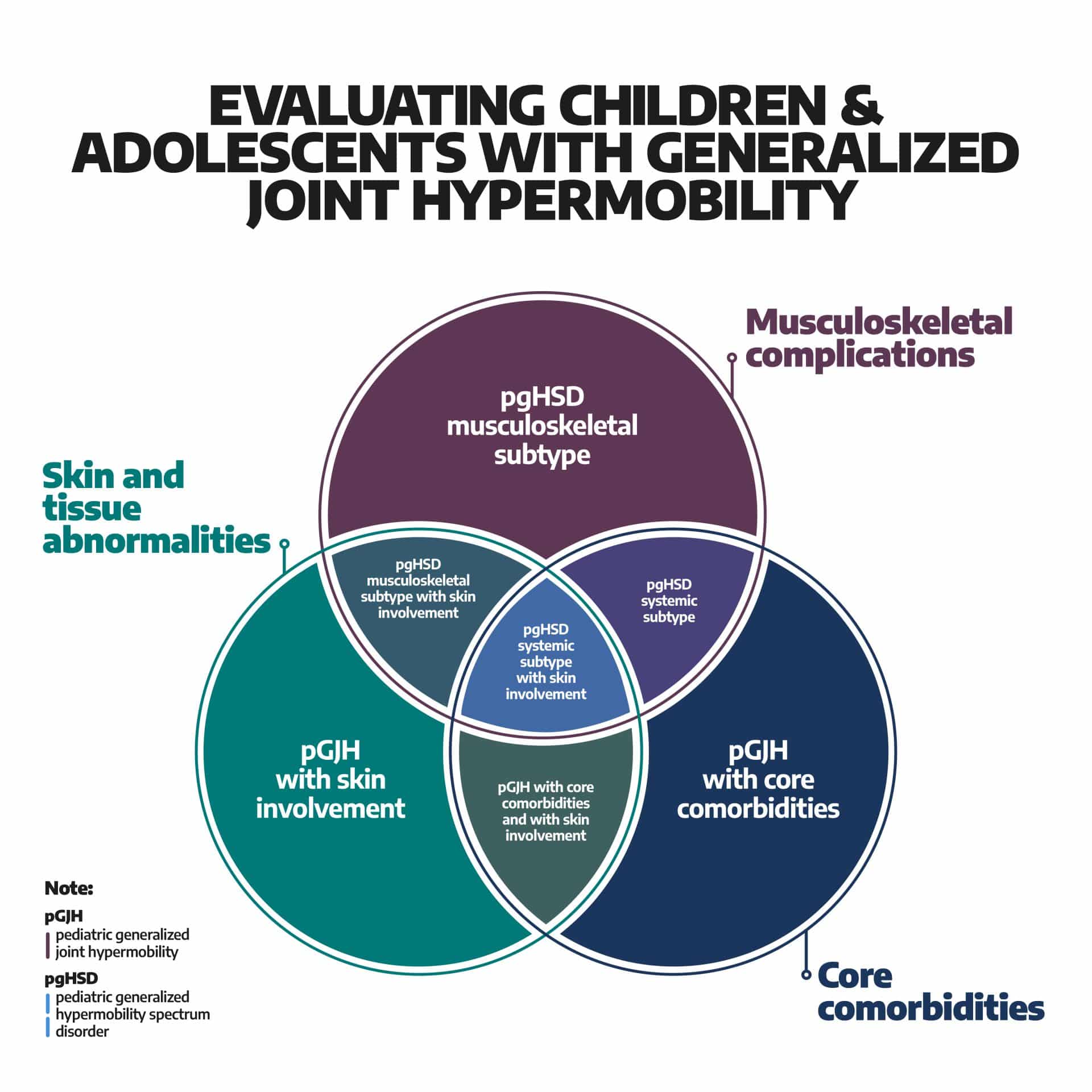
5 to skeletal maturity: We use the paediatric framework with your paediatrician or rheumatologist. A Beighton score of 6 out of 9 or more suggests generalised joint hypermobility. From here, the framework assesses whether there are musculoskeletal complications, core comorbidities (pain, fatigue, gut issues, dysautonomia, anxiety), and/or skin and tissue abnormalities. Children can move between categories as they grow, get stronger, or as symptoms change.
After skeletal maturity (around 16 to 18): Once they have stopped growing, the adult 2017 criteria can be used. This is when a diagnosis like hypermobile Ehlers-Danlos syndrome (hEDS) might be considered. Please note this criteria is expected to change in December 2026.
Its not just about the joints
This is something a lot of families do not realise until they are deep in the process. Connective tissue is everywhere in the body. So when hypermobility is symptomatic, it can show up in more places than you would expect.
Recent research has highlighted links between hypermobility and:
Bladder and gut function: One study found children with bedwetting were significantly more likely to have joint hypermobility (Derakhshan et al. 2025, BMC Pediatrics). Constipation, IBS-type symptoms, delayed toileting, and holding on too long are also common patterns. Connective tissue laxity can affect the pelvic floor and gut wall, not just the joints.
Sleep: Hypermobile adolescents showed more nighttime movement than peers (Schubert-Hjalmarsson et al. 2025, Pediatric Rheumatology). Restless legs, difficulty settling, and crashing by end of week are things we hear about regularly.
Fatigue: The same Swedish study found that fatigue in hypermobile teens was driven by pain catastrophising (the fear and worry around pain), not by how much they moved. The effect size was large. The psychological piece is central, not an add-on.
Autonomic system: Some children experience dizziness on standing, difficulty with temperature regulation, nausea, or dry eyes. This is sometimes called dysautonomia, and in more significant cases, postural orthostatic tachycardia syndrome (POTS). Management includes hydration, salt intake, exercise rehab, and identifying and managing triggers.
Foot posture: Flat feet in younger children are frequently a normal expression of developmental foot and ankle flexibility. A 2025 study found this largely reduces with age (Martinez-Sebastian et al., Journal of Paediatrics and Child Health). However if kids have pain or fatigue, check in with your podiatrist/physio.
Emotions: Anxiety, frustration, social withdrawal, and fear of movement or re-injury are common in kids with pain. CBT and graded activity exposure programs are effective alongside physical rehabilitation (Clark et al. 2024, Rheumatology International).
What tips the balance?
Hypermobility on its own does not usually cause problems. Symptoms tend to pop up when the load on the body outweighs the child’s capacity to cope.
Things that add load: growth spurts (especially puberty, when bones grow fast and muscles need to catch up), deconditioning (even a couple of weeks off activity can make a difference), transitions (starting school, moving from primary to high school), poor sleep, sickness, injury, surgery, and major life changes or stress.
Things that build capacity: strength through enjoyable activity, good balance and body awareness, good sleep routines, gradual loading over time, feeling confident in their body, keeping up and moving with friends, and a supportive environment at home and school.
We cannot change the hypermobility itself. But we can absolutely change the factors around it.

Many of the kids we see follow a pattern that builds on itself. It starts with the biomechanics: flexible tendons and lots of ankle movement means less spring for running and hopping. A few hops is fine. But repetitive, sustained tasks fatigue quickly because every push-off costs more energy. So running, because it is hard, doesn’t build fitness the way it does for other kids. They struggle to keep up with friends. Sport becomes less fun. They pull back. And the cycle deepens.
“Symptomatic” does not have to mean pain. It can mean fatigue, not keeping up, or not building skills as they grow. And this is why interrupting early matters so much. We do not wait for pain before we step in.
A word on handwriting and school
This is one of the most common concerns we hear from families. Children can spend up to a third of the school day on handwriting tasks (Schneider et al. 2022), and for kids with hypermobile hands and wrists, this can be genuinely hard.
What we often see is hand pain and fatigue from writing, reduced grip strength and finger control, and compensating grasp patterns (like wrapping the thumb over the pencil to create stability). Wesley et al. (2022, American Journal of Occupational Therapy) documented that these children have reduced grip strength, reduced in-hand manipulation, and reduced finger dexterity. Over time, this leads to writing avoidance and reduced output, which creates learning gaps if not supported. Parents in Wesley et al.’s 2021 study reported significant concerns about the impact on their child’s education.
The good news is there are practical things that help: pen grips, angled writing surfaces, keyboard or voice-to-text alternatives, wrist and hand splints (Wesley et al. 2024 scoping review mapped the OT strategies), hand strengthening exercises, and pacing with rest breaks. An occupational therapist can identify the specific strategies that will work best for your child. It is also worth asking about school accommodations like extra time for written assessments. Do not wait until the learning gaps are established.
What about flat feet and orthotics?
This comes up in almost every parent conversation, so it is worth addressing directly.
Flatter feet in younger children are frequently a normal expression of developmental foot and ankle flexibility. Martinez-Sebastian et al. (2025) studied 196 children aged 5 to 10 and found that foot posture was significantly correlated with foot and ankle hypermobility, and this naturally reduces with age. The Evans et al. Cochrane Review (2022) found no evidence supporting routine orthotics for asymptomatic flexible flat feet. So if your child has flat feet, no pain, and no functional issues? The evidence does not support orthotics.
However, when there IS pain or fatigue, the picture changes. Peterson et al. (2018, Journal of Foot and Ankle Research) found emerging evidence for prefabricated orthotics improving gait and dynamic balance in children with hypermobility and lower limb pain. Maarj et al. (2023) found custom orthotics reduced pain and improved quality of life over three months. The key is combining orthotics with a tailored strengthening program. It is not orthotics instead of exercise. It is orthotics alongside exercise.
So the answer is not “orthotics for everyone” or “orthotics for no one.” It depends on what is happening for your child.
What actually helps?
Stay active. This is the single most important thing. Muscles support joints. But it has to be something they enjoy. We need to build physical capacity in a way that is achievable, starting with the movement they love and building from there. Even replacing some sitting time with light activity is a meaningful first step.
Address the psychological. Fear of movement and worry about pain drive fatigue more than the hypermobility itself. Schubert-Hjalmarsson et al. (2025) found fatigue correlated with pain catastrophising, not activity levels. The effect size was large. Building confidence matters as much as building strength. CBT and graded activity exposure are effective, especially within multidisciplinary settings (Clark et al. 2024).
Look at the bigger picture. Sleep, gut health, bladder function, autonomic symptoms, emotional wellbeing. No single profession has the full picture. A multidisciplinary approach with physio, OT, psychology, and sometimes dietetics or continence support gives your child the best support.
Reassess over time. Do not rely on a one-off assessment. Their body is changing. Regular check-ins let us adjust the plan as they grow.
Listen to your child. Research consistently shows that children are better reporters of their own pain, fatigue, and quality of life than we sometimes give them credit for. International consensus (Quinlan et al. 2025) ranked child-reported measures above parent-reported in every domain. From around age 8, wherever possible, we should be asking the child first.
And parents, you matter too. You are the ones noticing the subtle changes at home, the behavioural shifts, the things your child cannot yet put into words. Both perspectives are essential.
When to Check in
These signs do not always mean there is a problem. But they are worth exploring with a professional who knows this space:
Trust your gut. You know your child best.
Take home message
Being bendy is common and usually completely normal in kids. Hypermobility only matters when it starts causing symptoms or limiting what your child wants to do. And “symptomatic” does not have to mean pain. It can mean fatigue, not keeping up, or not building skills as they grow.
We do not rush to diagnose in childhood because things change. But we do not wait and see either. We actively support your child to move, play, and learn. We focus on building capacity, keeping kids active, interrupting that downward spiral early, addressing the psychological and systemic factors, supporting handwriting and school participation, and reassessing as they grow.
If you are worried, reach out. If your child is bendy and thriving, celebrate their amazing body. And if they are somewhere in between, know that there is support available and things can get better.
You are the expert in your child. We are just here to help.
References:
Tofts et al. (2023). Pediatric joint hypermobility: a diagnostic framework and narrative review. Orphanet Journal of Rare Diseases.
Ituen et al. (2025). Age- and sex-related changes in joint hypermobility over two years. BMC Musculoskeletal Disorders.
European Journal of Pediatrics (2024). Variability of joint hypermobility in children: a meta-analytic approach to set cut-off scores.
Schubert-Hjalmarsson et al. (2025). Physical activity patterns in adolescents with HSD/hEDS. Pediatric Rheumatology.
Derakhshan et al. (2025). Joint hypermobility and primary nocturnal enuresis. BMC Pediatrics.
Martinez-Sebastian et al. (2025). Foot posture, foot/ankle tests, and hypermobility in children. Journal of Paediatrics and Child Health.
Lee et al. (2025). Parents’ experiences of pain communication in paediatric rheumatology. Patient Education and Counseling.
Quinlan et al. (2025). Outcome measures for children with hypermobility and lower limb pain. Clinical Rheumatology.
Wesley et al. (2022). Hand impairment and function in children with heritable disorders of connective tissue. American Journal of Occupational Therapy.
Wesley et al. (2021). Impact of heritable disorders of connective tissue on daily life of children: Parent perspectives. Journal of Paediatrics and Child Health.
Wesley et al. (2024). Conservative management of hand impairment in children with heritable disorders of connective tissue: A scoping review. Physical & Occupational Therapy in Pediatrics.
Schneider et al. (2022). A scoping review of grasp and handwriting performance in school-age children. Physical & Occupational Therapy in Pediatrics.
Peterson et al. (2018). Physical and mechanical therapies for lower limb symptoms in HSD and hEDS. Journal of Foot and Ankle Research.
Maarj et al. (2023). Impact of podiatric intervention on QoL and pain in children with hypermobility. IJERPH.
Evans et al. (2022). Cochrane Review: Foot orthoses for paediatric flexible flatfoot.
Clark et al. (2024). Psychological interventions for HSD and EDS. Rheumatology International.
normalbones.com: Pediatric bone x-ray reference database.
")
")
")
")
 (1)")
 (1)")